
Episode 77- Rabies immune globulin dose rounding
Episode Summary:
Want to save your site and your patient money while at the same time reduce drug waste? Listen now for one tip on how to do just that.
Show Notes:
Key Points:
“Rabies immune globulin dose rounding”:
– Rabies post-exposure prophylaxis (PEP) involves thorough wound care + administration of the rabies vaccine and rabies immune globulin (RIG). RIG is dosed at 20 IU/kg based on actual body weight and it’s infiltrated around the wound if possible, with the rest of the dose being given IM
– RIG can cost up to $6,000 per course and it can fall victim to drug shortages, so rounding to the nearest vial size to prevent waste and reduce cost just makes sense. One group of Pharmacists set out to describe their site’s dose rounding strategy for RIG to the nearest vial size to prevent waste and to save money
– In this multi-center, retrospective, observational study they compared patients who received RIG at doses rounded to the nearest vial size compared to those who did not have their doses rounded to the nearest vial size over the span of 11 years. The authors based cost calculations on rounding to the nearest 300 IU/1 mL vial ($804.53 per 300 IU vial)
– They included data from 426 patients. Overall, 373 (~ 88%) of patients had their dose rounded to the nearest vial size and 54 (~12%) did not. Of the 373 patients who had their dose rounded, 180 patients had their dose rounded down and 193 cases had their doses rounded up. Only 4% of patients got a dose that was less than 90% of the actual calculated dose, and only 13% of patients had a dose that was > 110% of the calculated dose
– They found that by rounding the doses down in those 180 patients, they saved 180 300 IU vials, with a direct cost savings of over $144,000. It also saved over 40,000 IU that would have been wasted from partial vial use had the dose not been rounded
– Approximately 55,000 Americans need rabies PEP every year, and if we extrapolated this data out to the entire nation we could save over 27,000 300 IU vials and about $22 million in direct healthcare costs each and every year
Source: Acquisto NM, et al. Am J of Emerg Med. 2022
Please click HERE to leave a review of the podcast!
Transcript:
Hello and welcome to Episode 77 of ER-Rx- a podcast tailored to your clinical needs. I’m your host, Adis Keric, and in this week’s Fresh Fruit series, we’re gonna be talking about saving your hospital and your patient money while at the same time reducing waste. We’re gonna do this by discussing a study published by a group of very smart pharmacists in the American Journal of Emergency Medicine in May of 2022. The study is entitled; “Assessment of rabies immune globulin dose rounding at a university health system.”
We all understand how dangerous rabies is– killing almost 100% of people once symptoms start. But rabies post-exposure prophylaxis (PEP) is also almost 100% effective at preventing disease. PEP involves thorough wound care along with giving patients the rabies vaccine and rabies immune globulin (RIG). Guidelines recommend giving RIG within 7 days of the first rabies vaccine, but ideally, we want to give it at the same time as the first dose of the vaccine. It’s dosed at 20 IU/kg based on actual body weight and it’s infiltrated around the wound if possible, with the rest of the dose being given IM in a limb opposite from where the vaccine was given.
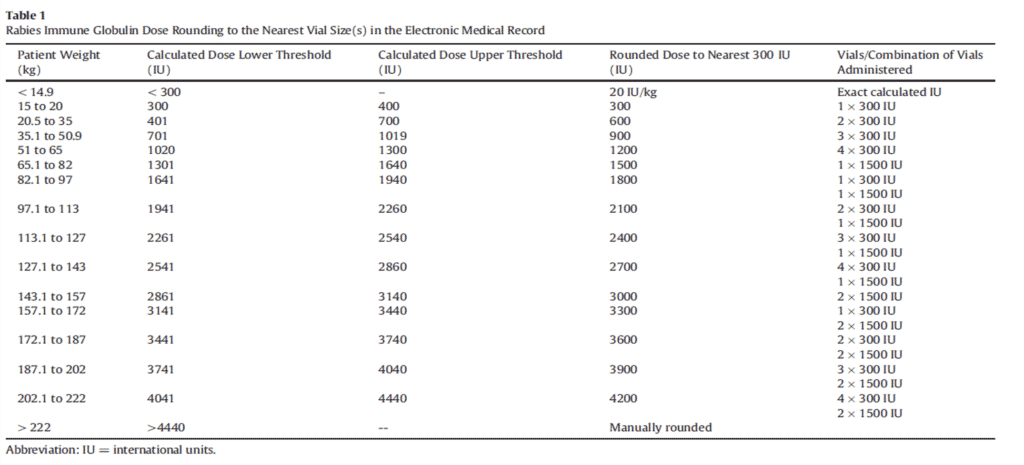
The authors point out that RIG can cost up to $6,000 per course, depending on insurance and pricing specific to each institution, and along with the cost, this agent can also fall victim to drug shortages. So rounding to the nearest vial size to prevent waste and reduce cost just makes sense- and as far as we know, it hasn’t really been studied before. Which is where this study comes in. The purpose of this study was to describe the site’s dose rounding strategy for RIG to the nearest vial size to prevent waste and to save money. They actually developed an automatic rounding algorithm within the electronic medical record- making it super easy for the verifying pharmacist. Check out Table 1- if you want to do something similar at your site to get an idea of how doses were rounded. I’ll post an image of the algorithm onto the ERRx Podcast Instagram page and onto errxpodcast.com.
This was a multi-center, retrospective, observational study looking at patients who received RIG at doses rounded to the nearest vial size compared to those who did not have their doses rounded to the nearest vial size over the span of 11 years. The authors calculated direct cost and units saved or wasted for each group, basing cost calculations on rounding to the nearest 300 IU/1 mL vial ($804.53 per 300 IU vial). They have a great example of how they calculated cost and units saved in the paper- which I highly encourage you to read.
They included data from 426 patients. Overall, 373 (~ 88%) of patients had their dose rounded to the nearest vial size and 54 (~12%) did not. Of the 373 patients who had their dose rounded, 180 patients had their dose rounded down (by a median of 77 IU) and 193 cases had their doses rounded up (by a median of 76 IU). Only 4% of patients got a dose that was less than 90% of the actual calculated dose, and only 13% of patients had a dose that was > 110% of the calculated dose. Remember that as a general rule, most pharmacists and institutions allow dose rounding if the dose is within 10% of the actual calculated dose.
They found that by rounding the doses down in those 180 patients, they saved 180 300 IU vials, with a direct cost savings of over $144,000. It also saved over 40,000 IU that would have been wasted from partial vial use had the dose not been rounded.
Given the very low incidence of rabies in the US, the study was underpowered to detect differences in actual rabies infections between the two groups. But there were no documented cases of rabies in the entire region during the entire study period—so we can rest assured that slightly rounding doses down did not lead to more positive rabies cases- which is no surprise.
The authors did a fantastic job making this argument in their discussion section. In a nutshell, although the CDC doesn’t endorse any RIG conservation strategies and recommends it be given at the exact calculated dose – we have data that this is probably unnecessary. Actually, the WHO does endorse conservation strategies for RIG- saying that we should only use a quantity sufficient enough for wound infiltration—bypassing the need to inject the remainder IM. This is based on studies showing that intramuscular RIG administration doesn’t provide much systemic protection compared to infiltration around the wound and proper wound care— so rounding a dose down by at most a 300 IU vial is almost guaranteed to not be harmful to our patients.
Given that approximately 55,000 Americans need rabies PEP every year, if we extrapolated this data out to the entire nation, we could save over 27,000 300 IU vials and about $22 million in direct healthcare costs each and every year. Of course, there are many limitations to a retrospective study, but overall, I’d imagine this data can be extrapolated out to sites like yours and mine—all we’re looking at is rounding doses. Hats off to these authors because I am now personally in the works for developing our own, even slightly more aggressive, RIG dose-rounding algorithm. Please reach out to me on if you have any questions of what that will look like.
So, in conclusion, remember to round your RIG doses down to save money or up to the nearest vial size to reduce waste. We as pharmacists should be doing this every time we see an order for RIG- but if you want to simplify it- consider implementing an automatic dose rounding algorithm in the EMR if you can.
As always, thank you so much for your time, and thank you for wanting to learn more about pharmacotherapy. If you have comments or anything you’d like to add to this, or any other episode, please reach out to me — I’d love to respond to all comments and criticisms.
Before we go, I just want to give another huge shout-out to the prize winner in Canada who received some ER-Rx Podcast swag and some swag from our friend Jimmy Pruitt and the PharmSoHard Podcast. I also want to thank Dr. James Kempema- the creator of the PediSTAT app- for his generous donation of some free downloads for one of the most useful apps I have on my phone. If there are any new medical providers, residents, or students listening who also have an Android and don’t yet have this amazing app downloaded- please hit me up on the Instagram page and I’d be happy to give you a free download of the app on behalf of Dr. Kempema.
I appreciate all of you guys and I’ll see you next time.
References: